What is mandrax (methaqualone)?

Mandrax is a synthetic sedative drug that acts on the central nervous system, slowing brain activity and producing feelings of relaxation and euphoria. Known chemically as methaqualone, it has been a controlled substance in South Africa and most countries since the 1980s, yet remains widely available as a street drug, particularly in the Western Cape, Gauteng, and KwaZulu-Natal.
South Africa has one of the highest rates of mandrax use in the world, with the drug deeply entrenched in certain communities and regions. In South Africa, mandrax is typically smoked in combination with cannabis in a practice known as “white pipe”. The white pipe administration method is specific to this country and carries its own particular risks.
This article covers what mandrax is, how it works, what it does to the body over time, and what treatment for mandrax addiction involves.
What is mandrax and where does it come from?
Mandrax began as a legitimate pharmaceutical product before becoming one of the most widely misused sedatives in South Africa.
Methaqualone was first synthesised in India in 1951 by researchers Indra Kishore Kacker and Syed Husain Zaheer during research into antimalarial compounds. By the 1960s, methaqualone was being prescribed widely for insomnia, anxiety, and muscle tension under various brand names.
The brand “Mandrax” was a combination of methaqualone and the antihistamine diphenhydramine, marketed in Britain and South Africa. In the United States, the same drug was sold as Quaalude. By 1965, methaqualone had become the most commonly prescribed sedative in Britain.
Recreational misuse accelerated through the late 1960s and 1970s, and most countries withdrew methaqualone from legal use by the early 1980s. In the United States, methaqualone became a Schedule I controlled substance in 1984.
In South Africa, methaqualone is classified as a Schedule 7 substance under the Drugs and Drug Trafficking Act 140 of 1992, placing it in the highest category of controlled substances. Possession, manufacture, and supply all constitute criminal offences.
After methaqualone was banned globally, South Africa became one of the world’s largest markets for illicitly produced methaqualone, largely through supply networks sourcing anthranilic acid (the key chemical precursor) from India and China.
In South Africa, mandrax goes by several street names: “buttons”, “MX”, “lizards”, and “flowers”, though the most widely used reference is the method of smoking it, the “white pipe.”
How mandrax is used in South Africa
The dominant method of mandrax use in South Africa is the “white pipe” or “bottleneck”, a practice largely unknown outside this country. A tablet is crushed and mixed with cannabis, then loaded into the broken neck of a glass bottle and smoked. The method delivers a rapid onset of effects and simultaneously intensifies the impact of both substances.
Oral ingestion is also possible but far less common, given that illicitly produced tablets vary considerably in composition and purity. Street mandrax is typically found as small, round tablets in off-white, grey, or brown, or as a loose powder.
Purity in illicitly manufactured batches varies from around 30% to 70%, meaning users have limited ability to gauge the actual dose they are consuming. Effects from smoking last approximately one to two hours; oral ingestion produces effects lasting up to five hours or more.
How mandrax affects the brain and body
Mandrax works by enhancing the activity of GABA, the brain’s primary inhibitory neurotransmitter. GABA reduces neuronal activity across the central nervous system, producing calming, sedative effects. By binding to GABA-A receptors as a positive allosteric modulator, mandrax amplifies GABA’s dampening effect in much the same way as benzodiazepines or barbiturates, slowing communication across the brain and body.
What distinguishes methaqualone from other GABA-acting drugs is that it can also produce excitatory effects at certain receptor subtypes, making it a mixed modulator.
This combination of sedation and excitation contributes to the drug’s euphoric properties and is part of what makes it particularly reinforcing. Methaqualone also has a long elimination half-life of 20 to 60 hours. This means it remains pharmacologically active in the body well after the acute effects have passed, and repeated doses can accumulate faster than users anticipate.
The effects of mandrax
Mandrax produces a predictable set of short-term effects that become more serious with sustained use. When smoked via the white pipe, effects begin within minutes. Users typically describe the initial phase as intense relaxation and euphoria, followed by progressive sedation.
Short-term effects of mandrax include:
- Euphoria and a strong sense of calm
- Sedation and drowsiness
- Reduced anxiety and social inhibition
- Slowed heart rate and breathing
- Muscle relaxation
- Slurred speech and impaired coordination
- Numbness in the extremities
- Dry mouth, dizziness, and headache
The transition from intoxication to a dangerous level of sedation can happen quickly, and the margin between an intoxicating dose and a harmful one is narrower than many users realise.
Long-term or heavy mandrax use produces a separate, more serious set of effects:
- Cognitive impairment, including memory loss and difficulty concentrating
- Reduced muscle function and coordination
- Depression, mood instability, and persistent anxiety
- Delusions and disorientation
- Increased vulnerability to seizures
- Vision problems
- Social withdrawal, hostility, and behavioural changes
- Physical deterioration and weight loss
The risks of mandrax use
The most serious immediate risk of mandrax use is overdose. A dose of approximately 2,000mg can induce a coma when taken alongside alcohol, and a dose of 8,000mg can be fatal.
Overdose symptoms include delirium, convulsions, vomiting, and cardiac or respiratory arrest, all of which require emergency medical attention.
The white pipe method carries specific risks beyond those of mandrax alone. Both methaqualone and cannabis depress the central nervous system, and combining them intensifies the effects of each. Users who smoke the white pipe often redose as the initial high fades quickly, steadily increasing total exposure over a session.
Combining mandrax with any other CNS depressant, including alcohol, opioids, or benzodiazepines, significantly compounds the danger of respiratory depression — where breathing slows to a dangerous degree. This is the primary cause of death in sedative overdoses.
Mandrax addiction: How dependence develops
Dependence on mandrax can develop rapidly. The same mechanism that drives tolerance in benzodiazepines and barbiturates applies to methaqualone. GABA-A agonist tolerance can set in within days of regular use, though the precise timeline varies between individuals.
As tolerance develops, users need higher or more frequent doses to produce the same effect, deepening both physical and psychological dependence.
Physical dependence means the body adjusts to the presence of the drug and finds it difficult to function without it. Psychological dependence follows: the relief from anxiety and discomfort that mandrax provides becomes increasingly difficult to replicate without the drug.
The white pipe’s fast onset and brief duration reinforce compulsive redosing patterns. Since the initial high is short-lived, users return to the drug repeatedly across a session.
Mandrax dependence rarely exists in isolation. Many people who develop a dependence on methaqualone are also using cannabis, alcohol, or other substances, and a significant proportion have underlying mental health conditions, such as depression, anxiety, or a history of trauma, that predate the addiction. Addressing these co-occurring conditions is central to sustainable recovery.
Mandrax withdrawal: What to expect
Stopping mandrax after extended use should not be attempted without clinical supervision. Withdrawal from GABA-A depressant drugs, including mandrax, carries a risk of seizures and other dangerous complications without appropriate medical support.
Mandrax withdrawal symptoms typically begin within 12 to 24 hours of the last dose and reach their peak within 24 to 48 hours. The nervous system rebounds from the suppressive effects of the drug, producing effects broadly opposite to those of intoxication:
- Severe anxiety and agitation
- Elevated heart rate and blood pressure
- Insomnia and disturbed sleep
- Tremors and muscle cramps
- Profuse sweating
- Nausea and vomiting
- Seizures in severe or prolonged cases
Medical management of withdrawal involves medication to reduce symptom severity and continuous monitoring for complications. Detoxification from mandrax can take up to ten days, depending on the level and duration of use. Attempting to stop abruptly without clinical oversight can be life-threatening.
Mandrax in South Africa: What the data shows
Treatment admissions data from SACENDU (the South African Community Epidemiology Network on Drug Use) provide the clearest national picture of who is seeking help for mandrax dependence in South Africa.
The most recent data comes from two publications released by the South African Medical Research Council (SAMRC):
- SACENDU Phase 58 Research Brief (January to June 2025, published May 2026)
- SACENDU Annual Report Vol 26 (January to December 2024, published March 2026)
Mandrax usage statistics
In the first half of 2025, cannabis/mandrax accounted for 3% of primary treatment admissions nationally, rising to 7% when secondary use is included. Measured as either a primary or secondary substance, the breakdown by province shows how concentrated cannabis/mandrax use is in the Western Cape.
In the January to June 2025 reporting period, the breakdown of cannabis/mandrax as a primary substance of use by province was:
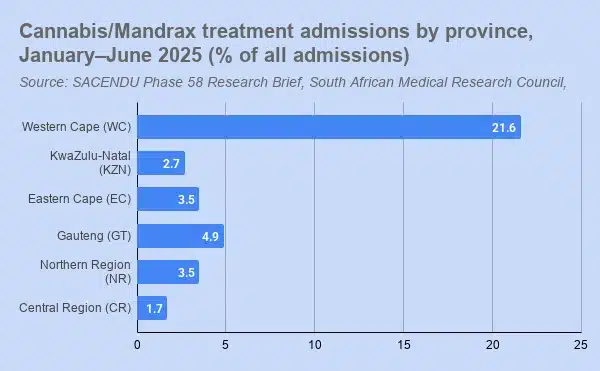
- Western Cape: 21.6%
- Gauteng: 4.9%
- Eastern Cape: 3.5%
- Northern Region (Mpumalanga and Limpopo): 3.5%
- KwaZulu-Natal: 2.7%
- Central Region (Free State, North West, Northern Cape): 1.7%
Mandrax in the Western Cape
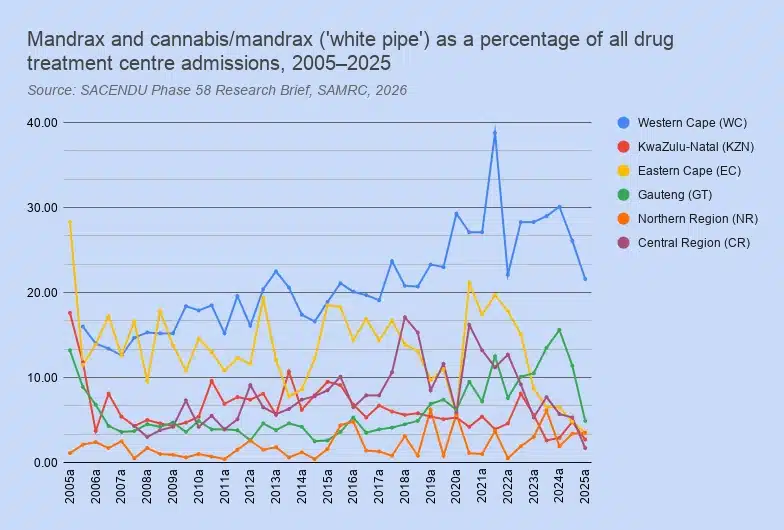
The Western Cape’s mandrax-related treatment admission rate is more than four times that of any other province, a gap that has held consistently across the full span of SACENDU data. Going back to 2006, the Western Cape has carried the highest cannabis/mandrax treatment rates in the country in every reporting period.
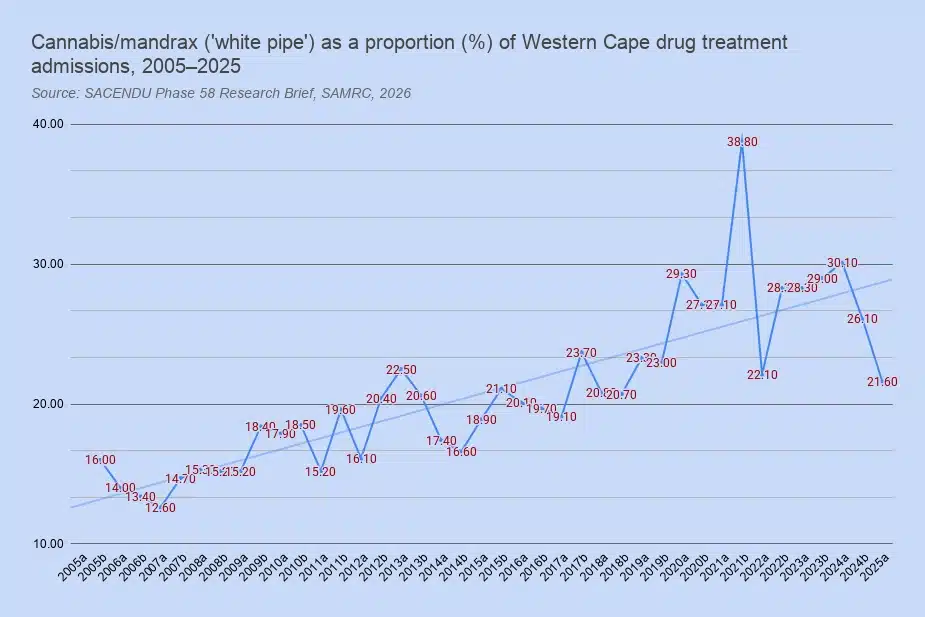
Over those two decades, rates more than doubled: from 14% of treatment admissions in 2006 to a high of around 30% by early 2024. A declining trend over the past three reporting periods has brought the rate back to under 22%.
Gauteng also showed a notable increase over the preceding decade before a sharp recent reversal. Rates rose from around 5% in the late 2010s to 16% by early 2024, then fell back to 5% in the first half of 2025.
Mandrax drug user demographics
The demographic profile of people in treatment for cannabis/mandrax use shows that admissions are predominantly male across all regions. In the Western Cape, the gender gap is narrower than for other substances, with 68% male and 32% female admissions for cannabis/mandrax in 2024.
The national mean age of patients presenting for cannabis/mandrax treatment is 31 years, compared to 22 years for those admitted for cannabis use alone, suggesting that white pipe use tends to establish itself in an older cohort.
Note: SACENDU captures treatment demand data, not population prevalence, so the figures almost certainly underestimate the true scale of mandrax use, particularly in areas where access to specialist treatment is limited.
Treatment for mandrax addiction
Effective treatment for mandrax dependence involves three phases: medical detoxification, residential rehabilitation, and sustained aftercare support.
Medical detox is the clinical priority. Because mandrax withdrawal carries a risk of seizures and cardiovascular complications, detoxification requires clinical supervision. At Houghton House, our medical detox programme is conducted on-site with 24-hour medical oversight, with duration depending on the level and duration of use. Where appropriate, we use medication to manage withdrawal symptoms and reduce the risk of complications.
Following detox, residential rehabilitation addresses the psychological and behavioural dimensions of addiction. Our drug rehabilitation programme incorporates individual counselling, group therapy, cognitive behavioural therapy (CBT), trauma-informed care, and 12-step facilitation, with treatment plans developed around each patient’s specific history and needs.
Because co-occurring mental health conditions are common among people with mandrax dependence, Houghton House’s dual licensing as both a rehabilitation facility and a registered psychiatric hospital means both addiction and psychiatric conditions can be assessed and treated within the same setting. Most rehabilitation centres are not equipped to provide this level of psychiatric care, which means underlying conditions can go unaddressed, increasing the risk of relapse.
After primary treatment, continuous care and aftercare provide the ongoing support that reduces relapse risk. Recovery from mandrax dependence is a sustained process, and the period following discharge from residential care is when support structures matter most.
Medical aid cover for mandrax treatment
Substance use disorders, including methaqualone dependence, are Prescribed Minimum Benefits (PMBs) in South Africa. All registered medical aids are legally required to cover addiction treatment. Because Houghton House holds dual licensing as a rehabilitation facility and a registered psychiatric hospital, patients can additionally claim for psychiatric services where co-occurring conditions qualify under psychiatric PMBs.
To find out what your scheme covers and how to access treatment, contact our admissions team directly, or visit our medical aid cover page for information on specific schemes, including Discovery, Bonitas, GEMS, and others.
Frequently asked questions about mandrax
What is the white pipe?
The white pipe, also called a bottleneck, is a method of using mandrax specific to South Africa. The user crushes a mandrax tablet and mixes it with cannabis. Then they load into the broken neck of a glass bottle and smoke directly through it. This method produces a rapid, intense onset of effects. It is considered particularly dangerous because it combines two CNS depressants and makes dosage control very difficult.
Is mandrax the same as Quaalude?
Both Mandrax and Quaaludes contain methaqualone as the active ingredient. Mandrax was the brand name used in Britain and South Africa, while Quaalude was the US brand name. The original Mandrax formulation also included the antihistamine diphenhydramine. Both were discontinued globally in the 1980s. The street drug known as “mandrax” or “buttons” in South Africa refers to illicitly manufactured methaqualone.
Is mandrax legal in South Africa?
No. Methaqualone is a Schedule 7 substance under the Drugs and Drug Trafficking Act 140 of 1992. Schedule 7 is the highest classification of controlled substance, meaning possession, use, manufacture, and supply are all criminal offences with no legal exceptions.
How quickly does mandrax addiction develop?
Tolerance to methaqualone can begin forming within days of regular use, with physical and psychological dependence following sustained use. The white pipe method’s fast onset and short duration tends to accelerate compulsive use patterns, as the brief high prompts frequent redosing.
Can you overdose on mandrax?
Yes. The margin between an intoxicating dose and a dangerous one is narrow. The risk also rises substantially when you mix mandrax with alcohol, cannabis, or other sedatives. Overdose symptoms include unconsciousness, convulsions, and cardiac or respiratory arrest. An overdose requires immediate emergency medical attention.
What does mandrax look like?
Legitimate pharmaceutical mandrax tablets no longer exist. Street mandrax in South Africa is typically found as small, round tablets. These can be off-white, grey, or brown. It can also come in the form of a loose powder. Colour, texture, and quality vary depending on the source and manufacturing process.
Where can I get help for mandrax addiction in South Africa?
Houghton House offers medically supervised detoxification and residential rehabilitation for methaqualone dependence in Johannesburg. Our clinical team can assess your situation and guide you through the admission process. Contact us to speak to our admissions team, or call us on 011 787 9142.