What is heroin? Understanding heroin addiction in SA
Understanding heroin addiction
Heroin is an illegal opioid derived from morphine, which is extracted from the opium poppy plant. Among the most addictive substances known, heroin can produce physical dependence after only a few uses, with withdrawal severe enough to require medical supervision.
In South Africa, heroin use has grown significantly over the past two decades and is now a leading driver of addiction treatment admissions in the Northern Region, KwaZulu-Natal, and Gauteng. South Africa’s heroin problem has distinctive features. Most heroin in the country arrives as brown powder and is typically smoked rather than injected. In inland provinces, it frequently circulates as ‘nyaope’, a street drug mixture containing heroin and cannabis.
This article covers what heroin is, how it works, what it does to the body, how dependence and withdrawal develop, and what treatment involves.
What is heroin, and where does it come from?
Heroin began as a pharmaceutical product before becoming one of the most widely misused drugs in the world. Morphine, heroin’s parent compound, was first isolated from opium in the early 19th century and became the dominant painkiller of its era.
In 1898, the pharmaceutical company Bayer synthesised diacetylmorphine as a supposedly non-addictive alternative to morphine, marketing it under the brand name “Heroin”. The name came from the German heroisch, meaning ‘heroic’, a reference to the powerful sensation it produced. The drug’s addictive potential became apparent quickly, and most countries had withdrawn it from medical use by the mid-20th century.
Heroin is no longer produced for medical use in most of the world. The illicit supply comes primarily from opium-producing regions in Afghanistan, which accounts for the majority of global production.
In South Africa, heroin typically arrives as brown powder, known on the street as “brown sugar”. White powder heroin and black tar heroin, more common in North American and some European markets, are less prevalent here.
Street names for heroin in South Africa include “unga”, “H”, “white”, and “smack”, though usage varies by region. In Gauteng and other inland provinces, “unga” is the most widely used term.
Heroin is classified as a Schedule 7 substance under the Drugs and Drug Trafficking Act 140 of 1992, placing it in the highest category of controlled substances in South Africa. Possession, manufacture, and supply are all criminal offences.
How heroin is used in South Africa
Heroin can be smoked, snorted, or injected. The route of administration affects how quickly effects arrive, how intense they are, and what risks each method carries. In South Africa, smoking is the dominant method, particularly in inland provinces.
- Smoking (‘chasing the dragon’): Heroin powder is placed on foil and heated from below; the vapour is inhaled through a tube. Onset is rapid, and the effects are intense, though slightly less so than with injection. Smoking is the most common method in South Africa.
- Injection: Heroin is dissolved and injected into a vein, producing an almost immediate rush. Injection carries the highest overdose risk and additional harms from needle use, including a significant risk of HIV and hepatitis C transmission.
- Snorting: Heroin powder is inhaled through the nose, producing a slower onset than smoking or injection. Less common in South Africa.
- Nyaope (also called ‘whoonga’ or ‘wunga’): A street drug mixture containing heroin as the primary active ingredient, typically combined with cannabis, and smoked. Nyaope is associated particularly with Gauteng, KwaZulu-Natal, and the Northern Region.
Street heroin varies considerably in purity and is frequently cut with paracetamol, starch, caffeine, or other substances. Users have no reliable way to gauge the actual dose in any given batch, which raises the risk of accidental overdose.
How heroin affects the brain and body
Heroin acts on opioid receptors distributed throughout the brain and body. Heroin’s primary effect is through the mu-opioid receptor, the subtype most closely associated with pain relief, sedation, and the release of dopamine in the brain’s reward pathway. By binding strongly to these receptors, heroin produces an intense rush of euphoria, followed by a prolonged state of warmth and sedation.
What makes heroin particularly reinforcing is the speed and intensity of this response. Smoked or injected, heroin reaches the brain within seconds and activates the reward pathway far more powerfully than natural stimuli or most prescription opioids. The brain records this activation as an exceptionally strong signal to repeat the behaviour, laying the neurological groundwork for dependence.
Heroin also suppresses the respiratory centres in the brainstem, which contain a high density of opioid receptors. As the dose increases, activation of those receptors slows breathing to a dangerous degree. Respiratory depression is the direct cause of death in heroin overdose.
The effects of heroin
The effects of heroin depend on the dose, route of administration, and the person’s level of tolerance. First-time users often experience nausea and vomiting alongside the euphoric effects. With regular use, tolerance to the euphoria develops rapidly, meaning users need increasing doses to achieve the same effect. Tolerance to respiratory depression develops more slowly, which raises the overdose risk as doses escalate.
Short-term effects include:
- Intense euphoria and a rush of warmth and well-being
- Sedation and drowsiness (“nodding off”)
- Reduced perception of pain
- Slowed heart rate and breathing
- Nausea and vomiting, particularly in newer users
- Constricted pupils
- Dry mouth and itching
- Impaired coordination and slurred speech
Long-term or heavy use produces more serious consequences:
- Physical dependence, with severe withdrawal when use stops
- Cognitive impairment, including problems with memory, concentration, and decision-making
- Damage to nasal tissue from snorting, and to veins from injection
- Significantly raised susceptibility to infection, including HIV and hepatitis C in people who inject
- Hormonal disruption and reduced libido
- Chronic constipation and gastrointestinal problems
- Lung damage from smoking
- Persistent depression and anhedonia (reduced capacity for pleasure)
- Deteriorating social relationships, employment, and physical health
Heroin overdose
Heroin overdose is a medical emergency. Breathing slows critically or stops when opioid receptors in the brainstem are overwhelmed. Heroin also suppresses the gag reflex, so an unconscious person is at risk of choking. An overdose can happen to anyone using heroin, including those with high tolerance. The risk rises sharply after any period of abstinence, when tolerance has dropped, but a person returns to a previously familiar dose.
Signs of a heroin overdose include:
- Slow, shallow, or stopped breathing
- Blue or grey lips and fingertips (cyanosis)
- Loss of consciousness or unresponsiveness
- Choking or gurgling sounds
- Pinpoint pupils
- Limpness
Naloxone (brand name Narcan) is an opioid antagonist that can reverse a heroin overdose within minutes, given as a nasal spray or injection. Naloxone displaces heroin from opioid receptors and restores normal breathing. Because naloxone’s effects are shorter-lived than heroin’s, a person may need more than one dose, and emergency care is still required even after successful administration.
If you suspect someone is overdosing on heroin, call emergency services (10177 or 112) immediately and give naloxone if available.
Heroin addiction: How dependence develops
Physical dependence on heroin can develop within days to weeks of regular use. Opioid tolerance sets in rapidly: the brain adapts to the drug’s presence by reducing its own opioid receptors, requiring larger doses to produce the same effect. As tolerance deepens, users take more of the drug more often, which strengthens both the physical and psychological hold of the addiction.
Physical dependence means the body has reorganised its chemistry around heroin’s presence. When a person stops using, the nervous system rebounds from chronic suppression and produces a severe withdrawal syndrome. Psychological dependence compounds this: the relief from pain, anxiety, and low mood that heroin provides becomes increasingly difficult to find any other way.
Heroin dependence rarely develops in isolation. A significant proportion of people who become dependent have a history of trauma, chronic pain, or untreated mental health conditions. Others begin with prescription opioid use and move to heroin as a cheaper or more accessible alternative. Addressing these underlying factors alongside substance use is central to sustained recovery.
Heroin withdrawal: What to expect
Heroin withdrawal is among the most severe withdrawal syndromes of any substance. For otherwise healthy adults, the acute phase is survivable, but its intensity drives a high rate of relapse without medical support. Attempting to withdraw without clinical supervision significantly increases that risk. Returning to heroin after any period of abstinence carries a high overdose risk because tolerance drops quickly.
Heroin withdrawal timeline
Symptoms begin within 6 to 12 hours of the last dose. Withdrawals reach peak intensity between 36 and 72 hours, largely resolving within 10 days. The progression follows a broadly predictable pattern:
- Early stage (hours 6 to 24): Anxiety, restlessness, yawning, runny nose, and mild muscle aches. Uncomfortable but manageable. Cravings intensify.
- Acute peak (days 1 to 3): The most medically critical phase. Severe muscle cramps, vomiting and diarrhoea, profuse sweating and chills, insomnia, agitation, elevated heart rate and blood pressure, and intense cravings. Clinical oversight is essential during this phase.
- Declining phase (days 4 to 7): Physical symptoms ease from their peak. Fatigue, disturbed sleep, mood disturbance, and cravings remain significant.
- Resolution (days 7 to 10): Acute symptoms largely resolve. Energy and sleep begin to stabilise, though mood can remain low.
- Post-acute phase (weeks to months): Fatigue, disturbed sleep, low mood, and intermittent cravings that can persist long after acute withdrawal ends.
Medical management targets the acute peak and declining phases. Opioid-based medications such as methadone and buprenorphine reduce cravings and withdrawal intensity. Non-opioid medications manage elevated heart rate, blood pressure, and specific symptoms. Clinical supervision throughout is essential.
Heroin in South Africa: What the data shows
Treatment admissions data from SACENDU (the South African Community Epidemiology Network on Drug Use) provide the clearest national picture of who is seeking help for heroin dependence in South Africa.
The most recent data comes from two publications released by the South African Medical Research Council (SAMRC):
- SACENDU Phase 58 Research Brief (January to June 2025, published May 2026)
- SACENDU Annual Report Vol 26 (January to December 2024, published March 2026)
Note: SACENDU captures treatment demand data, not population prevalence. This means the figures below underrepresent the true scale of heroin use in South Africa. This is particularly true in areas where access to specialist substance use treatment is limited.
Heroin addiction treatment statistics
- Heroin and other opiates comprised 7% of all treatment admissions nationally in the first half of 2025 — down from 10% in the preceding reporting period.
- Nationally, the mean age of persons admitted to treatment centres for heroin as their primary substance of use was 34 in January–June 2025.
- The most commonly reported route of administration in South Africa in the first half of 2025 continues to be smoking (69%), followed by injection (28%).
- Heroin/opiate admissions for persons under the age of 18 remain low nationally.
- Nationally, persons identifying as male accounted for the majority of heroin-related treatment admissions in the first half of 2025 across all regions.
Measured as either a primary or secondary substance of use, the provincial breakdown for heroin-related admissions to treatment centres in the first half of 2025 is as follows:
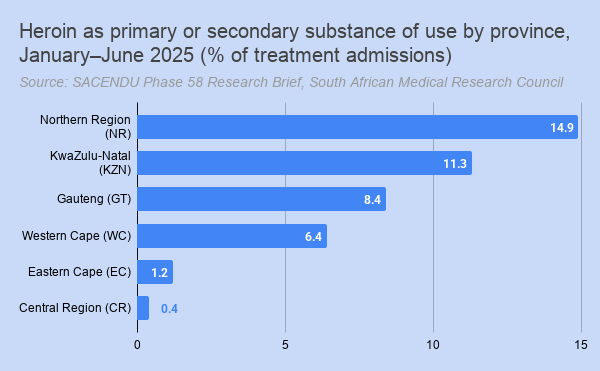
- Northern Region (Mpumalanga and Limpopo): 14.9%
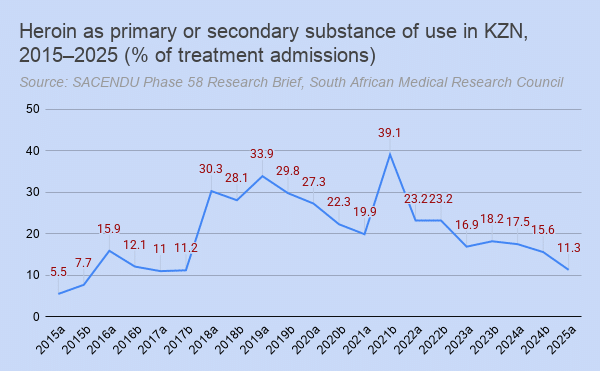
- KwaZulu-Natal: 11.3%
- Gauteng: 8.4%
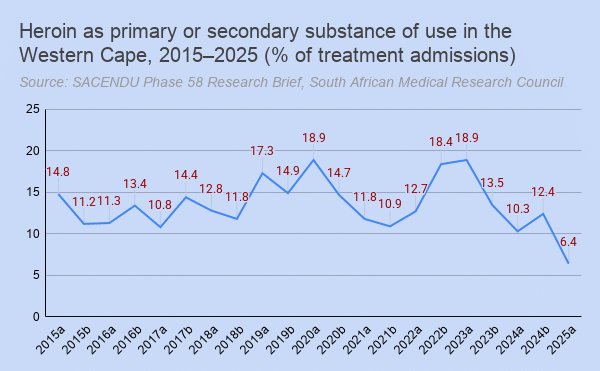
- Western Cape: 6.4%
- Eastern Cape: 1.2%
- Central Region (Free State, North West, Northern Cape): 0.4%
Unlike cannabis/mandrax, which is concentrated in the Western Cape, heroin treatment admissions are highest in the Northern Region (Mpumalanga and Limpopo), KwaZulu-Natal, and Gauteng.
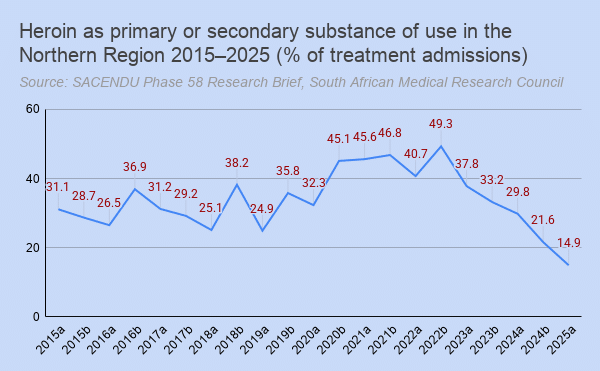
The Northern Region
The Northern Region has seen high heroin treatment rates throughout the full span of SACENDU data, reflecting long-established patterns of heroin use in Mpumalanga and Limpopo. Heroin-related admission rates reached a peak of 49.3% in the second half of 2022 before declining to a ten-year low of 14.9% in the first half of 2025.
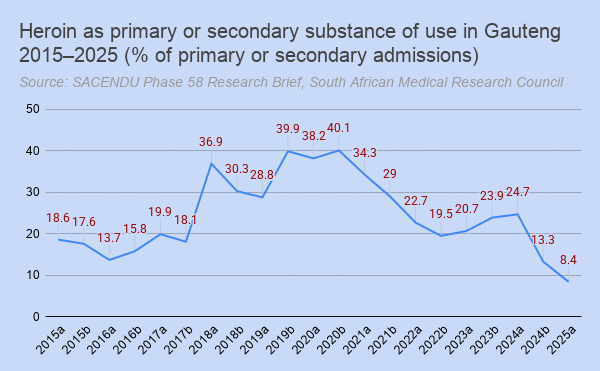
Gauteng
Gauteng’s heroin treatment rates have remained below 20% from 2015 through 2017, then jumped to 36.9% in the first half of 2018, a near-doubling in six months, before reaching a peak of 40.1% in the second half of 2020. Rates have since fallen sharply, reaching 8.4% in the first half of 2025.
KwaZulu-Natal
KwaZulu-Natal shows a similarly steep rise and fall to Gauteng: rates climbed to 39.1% in the second half of 2021 before declining to 11.3% in the first half of 2025.
Western Cape
Despite carrying the highest overall addiction treatment burden nationally, the Western Cape has maintained comparatively low heroin rates throughout, reaching a 10-year low of 6.4% in the first half of 2025.
Treatment for heroin addiction
Effective treatment for heroin dependence involves three phases: medical detoxification, residential rehabilitation, and sustained aftercare.
Medical detox is the clinical priority. Heroin withdrawal is severe, and the risk of relapse without medical support is high. Houghton House’s medical detox programme covers the acute peak of withdrawal over three days, with 24-hour medical oversight and medication used where clinically appropriate. The programme gets you through the most critical phase of the withdrawal timeline. Thereafter, ongoing symptom management continues within the residential (inpatient) rehabilitation programme.
Following detox, residential rehabilitation addresses the psychological and behavioural dimensions of addiction. Our drug rehabilitation programme includes individual counselling, group therapy, cognitive behavioural therapy (CBT), trauma-informed care, and 12-step facilitation, with treatment plans built around each patient’s specific history and needs.
Co-occurring mental health conditions are common among people with heroin dependence, including depression, anxiety, PTSD, and trauma histories. Houghton House’s dual licensing as both a rehabilitation facility and a registered psychiatric hospital means addiction and qualifying co-occurring conditions can be assessed and treated within the same admission. Few rehabilitation centres can provide this level of psychiatric care alongside addiction treatment.
After primary treatment, continuous care and aftercare provide the ongoing support that reduces relapse risk. The period following discharge is when support structures matter most, given the intensity of post-acute withdrawal and the elevated overdose risk that comes with reduced tolerance.
Medical aid cover for heroin treatment
Substance use disorders, including heroin dependence, are prescribed minimum benefits (PMBs) in South Africa. All registered medical aids are legally required to cover addiction treatment. Because Houghton House holds dual licensing as a rehabilitation facility and a registered psychiatric hospital, patients can additionally claim for psychiatric services where co-occurring conditions qualify under psychiatric PMBs.
To find out what your scheme covers and how to access treatment, contact our admissions team, or visit our medical aid cover page for information on specific schemes, including Discovery, Bonitas, GEMS, and others.
Frequently asked questions about heroin
What is heroin made from?
Heroin is derived from morphine, which is extracted from the seedpod of the opium poppy (Papaver somniferum). Morphine is chemically processed using acetic anhydride to produce diacetylmorphine, the chemical name for heroin. Illicitly produced heroin varies significantly in purity and is frequently cut with paracetamol, caffeine, starch, and other substances.
What does heroin look like?
In South Africa, heroin is most commonly found as a brown or off-white powder, known on the street as “brown sugar”. White powder heroin and black tar heroin are less prevalent in the South African market. Colour, texture, and purity vary depending on the source and degree of adulteration.
What is nyaope?
Nyaope is a street drug mixture containing heroin as its primary active ingredient, typically combined with cannabis, and smoked. Nyaope is associated particularly with Gauteng, KwaZulu-Natal, and the Northern Region and is a significant driver of heroin treatment admissions in those provinces.
How quickly does heroin addiction develop?
Physical dependence can develop within days to weeks of regular use. The speed depends on the route of administration, frequency of use, and individual factors. Smoked or injected heroin reaches the brain within seconds and tends to establish compulsive use patterns faster than slower-onset routes. Tolerance begins forming early, driving escalating use.
What are the signs of heroin addiction?
Signs of heroin dependence include:
- Continued use despite serious consequences
- Withdrawal symptoms between doses, including muscle aches, sweating, restlessness, and anxiety
- Increasing tolerance, requiring higher or more frequent doses
- Secretive behaviour around drug use
- Financial difficulties
- Significant changes in behaviour and social functioning
- Constricted pupils, drowsiness, and slurred speech are signs of active intoxication.
Can you overdose on heroin?
Yes. Heroin overdose occurs when breathing slows critically or stops, and can be fatal without immediate intervention. The risk increases significantly when heroin is combined with alcohol, benzodiazepines, or other sedatives, and after any period of abstinence when tolerance has fallen. Naloxone can reverse an overdose if given promptly. If an overdose is suspected, call emergency services immediately.
How long does heroin withdrawal last?
Acute withdrawal typically begins within 6 to 12 hours of the last dose, peaks between 36 and 72 hours, and largely resolves within up to 10 days. A post-acute phase of fatigue, disturbed sleep, low mood, and intermittent cravings can persist for weeks to months. Medical management significantly reduces the severity of acute withdrawal and the risk of relapse.
Where can I get help for heroin addiction in South Africa?
Houghton House offers medically supervised detoxification and residential rehabilitation for heroin dependence in Johannesburg. Our clinical team can assess your situation and guide you through the admission process. Contact us to speak to our admissions team, or call us on +27 11 787 9142.